

Fall 2025
Nutritional epidemiology studies have played a significant role in understanding the relationship between nutrient intake and human health, but there are many factors to consider to accurately interpret results.
The field of nutritional epidemiology aims to understand how dietary factors influence the development and prevention of various health conditions. Nutritional epidemiology has been invaluable in advancing knowledge on many food-related risks and benefits, such as how maternal folate supplementation in pregnancy reduces the risk of congenital neural tube defects, or vitamin A deficiency increases the risks of measles-related mortality. In nutritional epidemiology studies, researchers evaluate whether there are any associations (i.e., correlations) between particular foods or nutrients and the health condition(s) of interest. For example, if there is a correlation between a nutritional factor and a disease in multiple studies, and bias and confounding factors can be reasonably ruled out, this may provide evidence that the dietary factor can cause the disease.
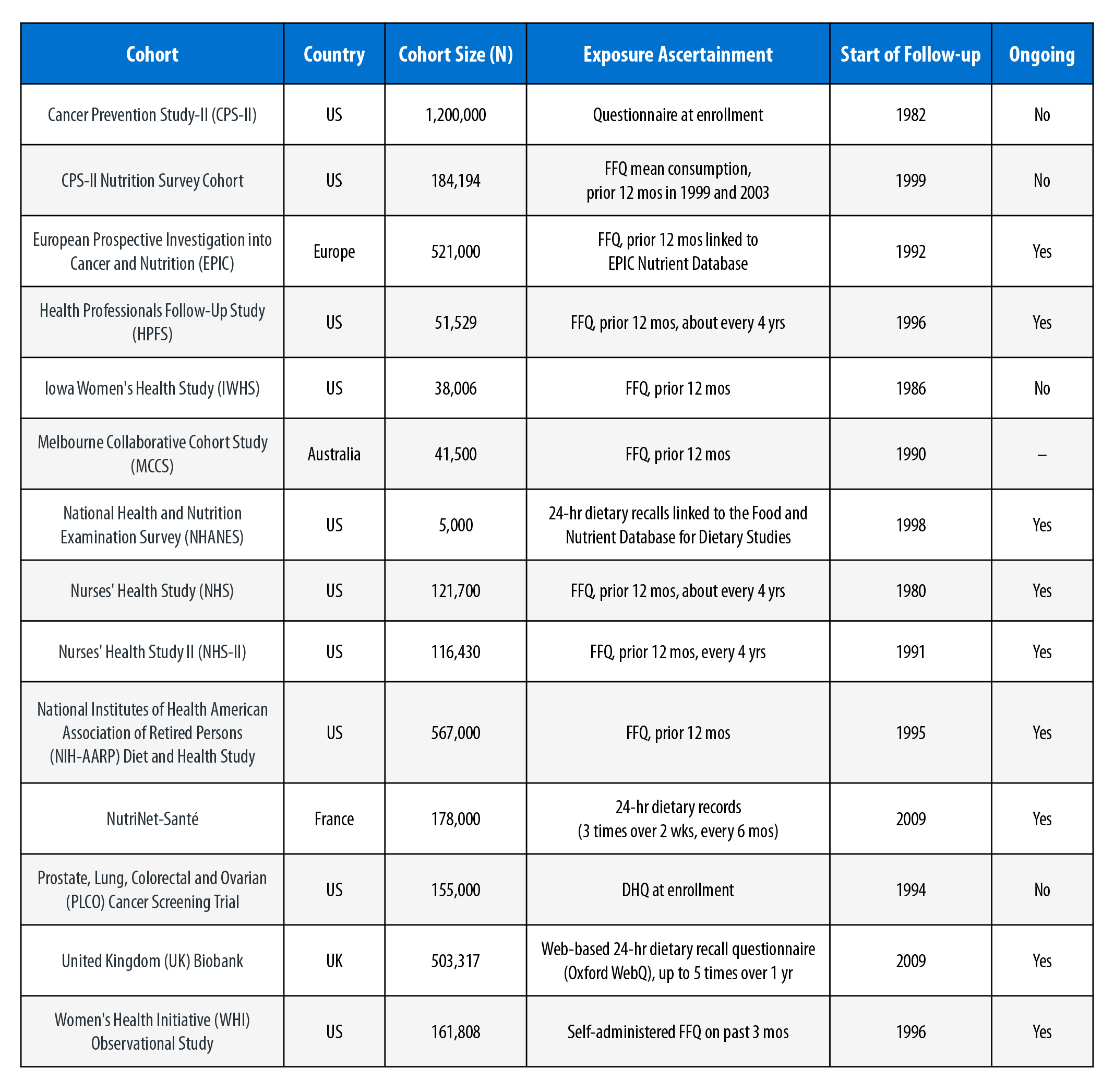
Information on health conditions is obtained using various methods, such as self-report, medical records, and health registries. In particular, food or nutrient intake can be estimated a number of ways, including information recorded from food diaries, 24-hour recall (i.e., people record what they ate in the last 24 hours), or food frequency questionnaires (FFQs) (i.e., people estimate the frequency with which certain items were consumed over a specific duration of time, such as the prior week). In addition, food and nutrient intake can be based on biochemical indicators, often in blood or urine from study participants. All approaches for assessing dietary intake are subject to some degree of error, and uncertainty can be introduced if estimates of the amount and frequency of food intake are not accurate. There are many sources of information for nutritional epidemiology studies, including several cohort studies (see Table).
When interpreting the results of nutritional epidemiology studies, one must keep in mind that people may misremember what they ate or may not accurately report portion sizes.”
Often the biggest challenge in nutritional epidemiology studies is accurately capturing dietary intake over the relevant time period of interest. Some studies assess dietary consumption only once or a few times over several years or decades. For foods or beverages for which consumption can vary over time, assuming a constant consumption pattern, sometimes over decades, may not reflect actual consumption patterns. Furthermore, when interpreting the results of nutritional epidemiology studies, one must keep in mind that people may misremember what they ate or may not accurately report portion sizes. Recall of dietary consumption over longer periods (e.g., a year) is less accurate than recall of information over shorter time periods (e.g., 24 hours). Moreover, social desirability bias can occur when people overreport eating what they perceive as healthy foods and underreport what they perceive as unhealthy foods. There are also many factors associated with food intake, such as exercise, socioeconomic status, and culture, which may explain associations with health outcomes that have been attributed to food intake. For example, a study might find an association between drinking alcohol and lung cancer; however, if people who drank alcohol were more likely to smoke in that study, and if the researchers did not control for smoking in their analysis, it could be smoking and not alcohol consumption that increased lung cancer risk.
Another issue with nutritional epidemiology studies is reverse causation. Often people with a certain health condition will change their diet after being diagnosed with a specific health outcome. For instance, someone who has been diagnosed with diabetes may reduce their intake of sugar and increase their intake of artificial sweeteners. In this example, it was not the increased intake of artificial sweeteners in the diet that caused diabetes, but rather the diabetes diagnosis that caused the change in diet.
Nutritional epidemiology can provide valuable insights into the relationship between consumption of specific foods or nutrients and health outcomes. The results of these studies, however, need to be carefully interpreted in the context of the quality of the study, particularly with respect to the quality of the dietary exposure assessment. In addition, continued support for long-term follow-up of ongoing studies is important to provide evidence on chronic health conditions that may take decades to develop.
These cohorts range in size from 5,000 to over 1,000,000 individuals. Exposures were measured in a number of ways. Several cohorts began collecting information in the 1980s, and most are still collecting information on participants. (References for cohort studies are provided below.)
The authors can be reached at Julie.Goodman@gradientcorp.com and Denali.Boon@gradientcorp.com.
American Cancer Society. 2025a. “Cancer Prevention Study II (CPS-II).” Accessed on September 11, 2025, at https://www.cancer.org/research/population-science/cancer-prevention-and-survivorship-research-team/acs-cancer-prevention-studies/cancer-prevention-study-2.html.
American Cancer Society. 2025b. “Cancer Prevention Study II (CPS-II) Nutrition Survey.” Accessed on September 11, 2025, at https://www.cancer.org/research/population-science/cancer-prevention-and-survivorship-research-team/acs-cancer-prevention-studies/cancer-prevention-study-2.html.
Brigham and Women’s Hospital; Harvard Medical School; Harvard T.H. Chan School of Public Health. 2025a. “Nurses’ Health Study (NHS).” Accessed on September 11, 2025, at https://nurseshealthstudy.org/.
Brigham and Women’s Hospital; Harvard Medical School; Harvard T.H. Chan School of Public Health. 2025b. “Nurses’ Health Study II (NHS II).” Accessed on September 11, 2025, at https://nurseshealthstudy.org/.
Cancer Council Victoria. 2025. “Overview of the Melbourne Collaborative Cohort Study (Health 2020).” Accessed on September 11, 2025, at https://www.cancervic.org.au/research/our-research/epidemiology/health_2020/health2020-overview.
Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS). 2025. “National Health and Nutrition Examination Survey (NHANES).” Accessed on September 11, 2025, at https://www.cdc.gov/nchs/nhanes/index.html.
Harvard T.H. Chan School of Public Health. 2025. “Health Professionals Follow-Up Study (HPFS).” Accessed on September 11, 2025, at https://hsph.harvard.edu/research/health-professionals/.
International Agency for Research on Cancer (IARC). 2025. “European Prospective Investigation into Cancer and Nutrition (EPIC-Europe study).” Accessed on September 11, 2025, at https://epic.iarc.fr/.
National Cancer Institute (NCI), Division of Cancer Control and Population Sciences. 2023. “Iowa Women’s Health Study (IWHS).” In Cancer Epidemiology Descriptive Cohort Database (CEDCD). Accessed on September 11, 2025, at https://cedcd.nci.nih.gov/cohort?id=143.
National Cancer Institute (NCI), Division of Cancer Epidemiology and Genetics. 2025. “NIH-AARP Diet and Health Study.” Accessed on September 11, 2025, at https://dceg.cancer.gov/research/who-we-study/nih-aarp-diet-health-study.
National Cancer Institute (NCI), Division of Cancer Prevention. 2025. “Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO).” Accessed on September 11, 2025, at https://prevention.cancer.gov/research-areas/networks-consortia-programs/plco.
National Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI). 2025. “Women’s Health Initiative (WHI).” Accessed on September 11, 2025, at https://www.nhlbi.nih.gov/science/womens-health-initiative-whi.
NutriNet-Sante Study. 2025. “NutriNet-Sante Study.” Accessed on September 11, 2025, at https://info.etude-nutrinet-sante.fr/siteinfo/.
UK Biobank Ltd. 2025. “UK Biobank.” Accessed on September 11, 2025, at https://www.ukbiobank.ac.uk/.